THE MOVING BODY - Walking Gait Analysis (Part III): Gait Deviations
INTRODUCTION
In part one of this series of articles on walking, we covered the basics of the walk cycle, including its deconstruction. In part two, we added more detailed information on the muscles and mechanical structures that should engage in healthy locomotion.
In this piece, we will cover some of the most common deviations from the "standard" walk, and see both what happens when parts of the system fail, and how the body tries to adapt around it.
Walking deviations are usually classified by higher-than-normal energy requirements for moving and/or a slower speed that can impact daily life.
Deviated gaits are usually derived from the standard gait we've seen so far, and they obviously also exist on a spectrum. On one end, if the deviation gives little to no friction in daily life, it could just be seen as a personal variation of the gait. We all have little to mild variations in our walking gait based on our physical proportions, fitness level, and differences based on sex, age, weight, footwear, level of energy in that moment, mood, you name it.
On the other end of the spectrum, we can push the abnormality to the point where they interfere with daily life and people's well-being. Most of these deviations are not gait-impeding, as most people are still able to walk places. What happens in many cases like these is that the body will naturally adapt and work around weaknesses by changing its stance or using other muscles to try to replace the one that might not be working as intended. But the main issue with these compensation strategies is that the replacing muscles are often not able to sustain the workload needed for long periods of time, or are unable to recreate exactly what is needed. This can lead to higher-than-usual muscle fatigue and pain from overload, as a few examples. That said, some of these variations can be temporary if, for example, they are caused by a temporary injury or muscle fatigue.
In these variations we will cover, we will point out the main cause of dysfunction, compare it to the “standard“ gait and how it differs, and see how the body works around it.
/!\ This is not a medical article. It's simply a study of movement /!\
TRENDELENBURG GAIT
The Trendelenburg gait affects mostly the stance phase of the gait cycle. Due to a weakness in the support gluteus muscle, the body is forced to compensate with a larger-than-usual shift and rotation to the side.
STANDARD GAIT:
In a standard gait, during the phase of single-leg support, the support muscles of the hip (mainly the gluteus muscles) help stabilize the hip and keep it level to avoid the natural drop to one side that would occur the moment we remove the opposite leg as support. This hip stabilization helps avoid larger-than-necessary shifts side to side.

(single leg support)
Though causes can change, in people affected by Trendelenburg gait, we find a general weakness of these support muscles, which often affects one side, but it can happen on both. This gait variation can look slightly different depending on whether the gait is compensated or uncompensated. In an uncompensated Trendelenburg gait, we see a visible hip drop on one side, creating an exaggerated swing of the hips when the weight is put on the leg of the side/s affected. Excessive hip rotation during the stance phase is how we recognize this gait.

Source: https://youtu.be/olZYoe3gr2Q

Slow motion
In a compensated Trendelenburg, the body tries to keep the hips level by shifting and leaning with the trunk during the stance phase of the walk towards the supporting leg. This helps shift the weight on the side of the support leg and keeps the hips level, reducing the demands on the glute muscles and redirecting the efforts to the torso instead. If you compare the compensated and uncompensated Trendelenburg, you might notice that, although they can look different, if you isolate the movement of the hip relative to the side of the torso, the movement is quite similar. In either the is a compression of the torso on the affected side, in one with the hip moving towards the shoulder, while in the other with the shoulder moving towards the hip.

Slow motion
If the gluteus weakness happens on both sides, the effects of it can result in a waddling effect.
In normal day-to-day life, though obviously the causes differ, you can observe a similar compensated walking style even in healthier individuals. For example, when carrying a suitcase or a heavy object asymmetrically on one side. The torso naturally compensates in this case for the added weight that would otherwise drag the body to fall sideways during the stance phase. At the same time, it carries part of the effort away from the gluteus muscle, which might be unable to keep the hips level with the added weight. Something similar to this gait can be observed in obese/overweight people, due to the heaviness of the body and the likely lack of muscle strength required to maintain the hips leveled.
Some similar swing and lean side to side can also be visible when someone is exhausted. Usually, that comes with a stronger weight shift accentuation and excessive lean, in this case, not due to muscle weakness but muscle fatigue.
Source: https://youtu.be/wpfoARyxQpc
FOOT DROP / STEPPAGE GAIT / VAULTING GAIT
FOOT DROP
Foot drop gait affects the lower part of the gait during the phases of weight acceptance and leg advancement. It is generally caused by a weakness of the foot's dorsiflexors, mainly the tibialis anterior. The role of which, in simple terms, is to raise the foot at the ankle joint towards the ceiling.
Since a lack of proper dorsiflexion affects different parts of the gait, weakness in the tibialis anterior shows itself in different ways, both depending on which stage of the gait cycle we are in, and in the personal strategy the body adapts to work around this imbalance. Depending on which part of the gait this weakness hits we can classify gait as either steppage gait, if it hits predominantly during leg advancement, or foot drop, if it hits predominantly during weight acceptance. Though more often the two can come together.
STANDARD GAIT, leg advancement:
During the phase of leg advancement in a standard gait, the foot/ankle is generally dorsiflexed from mid-swing until terminal swing. This slight dorsiflexion helps ensure that the foot can clear the floor with minimal effort and without stumbling.
(leg advancement)
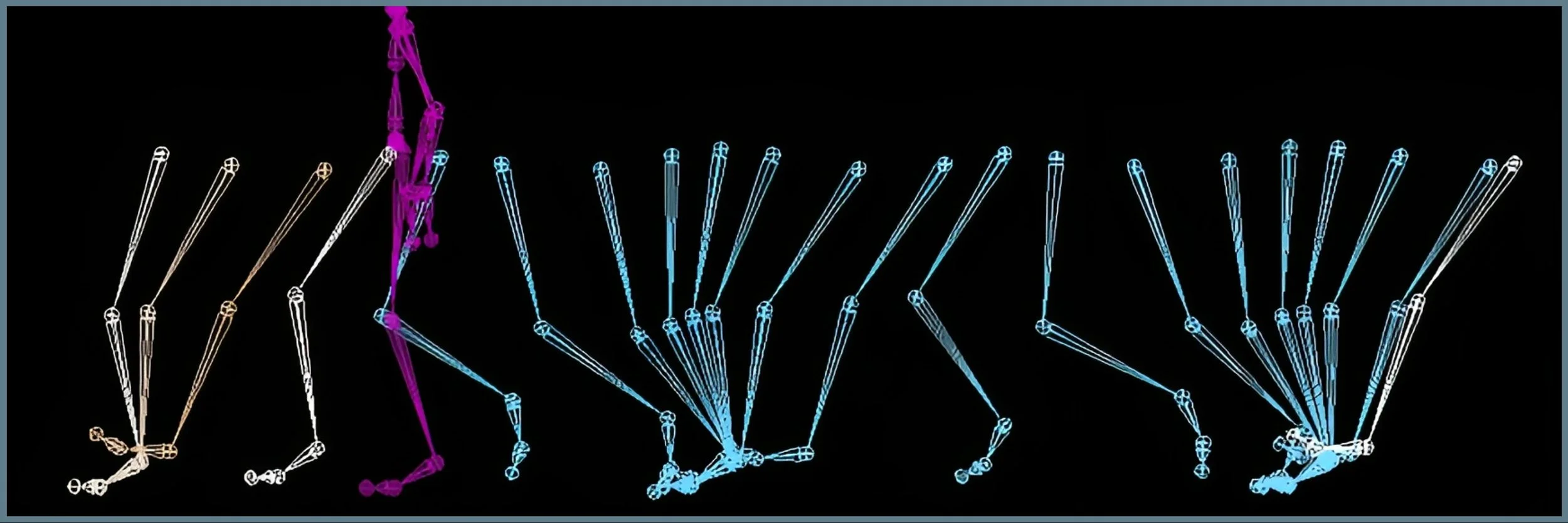
STEPPAGE GAIT
In people with a steppage gait, we can generally find two different compensations. Where the dorsiflexors are not helping, the hip and knee flexors compensate by lifting the whole leg higher to clear the floor. Externally, this can look a lot like someone who is stepping over an invisible obstacle. Lifting the whole leg instead of the foot obviously requires a lot more energy, making walking both slower and more tiring. In people whose dorsiflexors are truly almost completely dead or inactive, even with lifting the whole leg, it is not enough, and the toes still can drag across the floor while shifting the leg forward.

Source: https://youtu.be/7Ft1bUTzxkM
Slow motion
Another variation of a similar compensation happens when the person simply circumnavigates the leg towards the outside. This obviously allows to pass the leg in front without having to bend it, but at the cost of higher glute activation and slower gait.


Slow motion
On a similar strategy for clearing the leg, we find the vaulting gait, in which the person, during leg advancement, pushes up to the tip-toe of the weight-bearing leg to help create more space for the affected leg on the other side to move in front.

Slow motion
FOOT SLAP
STANDARD GAIT, weight acceptance:
From the moment the front heel touches the ground to the moment the foot is flat on the floor, the ankle dorsiflexor activates to ensure that the foot nicely and gently rolls towards the ground, rather than falling uncontrolled.


In people with foot drop/slap gait, the foot obviously lacks the control for a softer landing, and instead, the movements of the ankle simply follow through from the momentum of the upper part of the leg. This can mean a higher flexion before the foot touches the ground and a faster and harsher landing on the floor. This footfall can sometimes create a slapping sound, which gives this kind of gait adaptation its name.

Source: https://youtu.be/svcDcKw-o4I
Slow motion
Other times, the person can also reach the contact position with the toes pointing at the ground, almost like a tip-toe position, in which case the back part of the foot will be the part that tends to slam on the floor.
Source: https://youtu.be/cwZYuVB595Q
Slow motion
ANTALGIC GAIT
In the antalgic gait, the person has some form of pain in one leg that usually gets worse either under work or when weight is put on it. This results in what we generally see as a limping leg.
STANDARD GAIT:
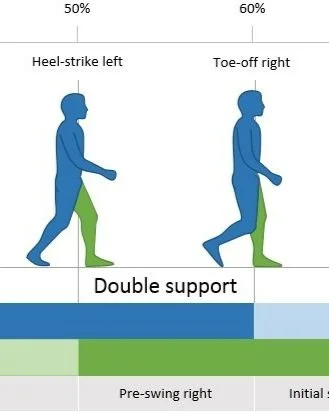
In a standard gait, the phase of single-leg support usually comprises 60% of the total gait cycle and brings the supporting leg from the front of the body to the back, where one leg must temporarily support the weight of the whole body.
The antalgic gait affects the stance phase of the cycle and might be one of the most common types of gait variation. It can have a great variety of sources, from a swollen ankle to muscle injury, a wound... Despite these variations in origin, they all generally result in a similar outcome, a difficult or painful stance phase on the injured leg. This gait is generally asymmetrical, meaning it affects only one side of the body, while the other side works normally.
To minimize the discomfort of the painful weight-bearing leg, the person tries to shorten as much as possible the time spent and the weight put on that side of the body. This can alter the body position in different ways, though conditions may vary depending on the type and location of discomfort and pain.

Source: https://youtu.be/rLyEZubc4tk

Slow motion
Some of the main points of adaptation might be:
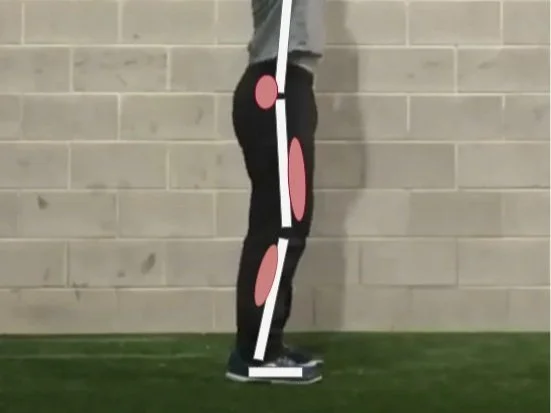
Joint mobility is reduced. Ankle, knee, and hip joints try to remain in a more stable, neutral position to avoid muscle aches. This means reduced or absent knee flexion during weight acceptance, reduced ankle flexion in contact position, and terminal swing. And a general reduction in the range of motion of the lower body.
Shorter stance phase. This is the main point of the antalgic gait: the time spent on the stance phase is reduced to a minimum. Because time for motion is limited, this generally also means a reduction in the amplitude of the movement. The antalgic gait tends to start with the contact position much closer to the body's center of gravity, and end with the terminal swing not much further behind the body as well.
"Falling" forward. Part of the normal gait cycle is falling forward towards the next contact position on the opposite leg. This is generally met with some resistance from the body that tries to control this fall for a smooth transition. In the antalgic gait, since the muscles of the injured leg cannot effectively resist gravity, the fall becomes a lot more accentuated, and the other side must work extra hard to catch the body and push it back up to normal height. Having to catch the body in this way can make the person lose all forward momentum as they try to recover. Having to start and stop continuously obviously makes walking a lot more tiring and energy expensive. (seen in the video above)
Manipulating the centre of gravity. To try to reduce the amount of pressure on the painful leg, the upper body can sometimes drop forward or adapt in other ways. This bending forward can look unrelated, but changing the shape of the torso also changes the centre of gravity in the body. Lowering the upper body naturally raises the center of gravity in relation to the leg, making it feel lighter on the lower part. This is a similar technique to falling forward, but instead, it's only the upper body falling to try to maintain the centre of gravity stable without using the leg muscles.
Using a cane. Using an object to support the body on the painful side is a very common method to transfer some of the weight bearing from the painful leg to the upper body.

Source: https://youtu.be/YcrIwtI4jl4
Here’s an example of a stylized antalgic gait used for a zombie character reference. You can read the short stance on one leg and the body falling forward.
ATAXIC GAIT
The ataxic gait is characterized by a wider stance, with irregular foot placement, timing of steps, and step length.
STANDARD GAIT:
Anticipation and predictability are often what make movements, whether we talk about the gait or any other, feel masterful and effortless. Often, when we repeat an action for long enough, like walking, the body anticipates what comes next, prepares to absorb the motion when necessary, and counteracts. This predictability makes sure that we prepare to "start" the next movement before we actually do. For example, the quadriceps of the legs generally start tensing moments before the contact of the foot with the ground in preparation for the weight of the body.
The ataxic gait is generally not developed by muscle weakness but by a lack of muscle coordination, which can be due to an impaired nervous system, whether the issue is spinal or cerebral. This can affect the signal of the action reaching the muscle, creating an unreliable muscle contraction (either too strong or weaker than expected), a lack of muscle coordination, and, by extension, uncoordinated motor action.
This lesion of the nervous system can have different causes and be serious and long-lasting, but it can also be temporary and be caused by drugs or inebriation. Most common of which, as you've probably seen around, is alcohol. Without going into details, alcohol is a nervous system depressant that can impair communication between neurons, leading to a lack of proprioception (the physical perception of your body in space).
Even before starting walking, due to the unreliable support and ability to maintain balance, the person will naturally gravitate towards a wider stance to increase the area of support under the body.
During gait, the steps tend to be wider, sometimes even lateral, sometimes moving forward a lot, sometimes not moving forward much.
Because of this unpredictability and instability, the body is forced to constantly react to what's happening rather than anticipating. Because the body is forced to react at the last split second to avoid falling, it often doesn't have the proper amount of time to project what the appropriate amount of strength needed to stabilize is. The reaction of the muscle then is often stronger and snappier than it should have been, leading to an overreaction of the body that might also create the need for another corrective reaction. This can lead one step forward to taking one step laterally or another step backwards, constantly trying to catch the body from falling, making moving straight and forward difficult and time and energy consuming.
This gait is also characterized by a cycle of stops and go. Where the person tries to walk forward, has a mistep, tries to adjust, and overcorrects. Leading the person to stop all forward momentum and take a brief pause to regain control of balance in standing, before attempting to lean forward and lunge once again. This is another layer of stress and energy that makes this gait slow and difficult.

Obviously, lack of coordination is the main issue with this gait, whether it comes from an impaired nervous system or…. not being good at walking yet. Children who are taking the first step can display basically the same signs: wider stance, difficulty moving forward, and overcorrecting movements. Though obviously nothing at all might be wrong with them.
As another example of the ataxic gait, and others that we listed, used as part of a character performance, let’s see how many you can spot in this video.
VARIATIONS ON THE NORMAL WALKING SPECTRUM
Most people don't walk "normally". Each one of us has a way of walking that, if really put under the microscope, can be as unique as a fingerprint or a person's handwriting. As mentioned at the beginning of the article, a person's walking style can include everything from the shape of their body to their mood, their energy, and so on. Just like the gaits we described, even on a more "healthy" range, our body naturally and rather quickly adapts to the circumstances and the environment, together with our physical makeup. As a finishing touch to this post, we can quickly cover some of the more common variations we can see around that are still part of a standard gait. See if you can spot them in the wild.
Toe-in/Toe-out: most people's feet are rarely straight forward when we walk. Very often, people’s feet naturally tend to fall either towards the outside (toe-out, more common) or inside (toe-in). This is often dictated by the prevalence of the muscles around the hips, which leads to the angle of the leg towards a specific side. This is usually symmetrical in the body, meaning that it tends to affect both legs.
Arm swing asymmetry: Most people have a favorite hand they use to do most things. This asymmetry of use generally leads to a physical asymmetry in development, both in strength and flexibility. Which can lead to the swings of the arms during walking being slightly asymmetrical.
Heel or Mid-foot strike: Different people tend to hit the ground in different ways. Some have their contact with the very end of the heel, while others hit their contact point more towards the middle. This can vary, even in the same person, depending on walking speed and footwear. When we walk fast and take big steps, we tend to more naturally hit the ground towards the heel, while shorter steps might tend to hit the floor towards the mid-foot. Footwear can also influence this, as some running shoes might be padded more heavily at the heel, making it more desirable to have the contact there. While other shoes are flatter at the bottom, making a heavy heel contact feel uncomfortable and pushing the person to have ground contact with a flatter foot.
Footwear alone can obviously have a big amount of influence on a person's walking gait, as most shoes themselves are designed to give comfort with a specific style of gait in mind, from weight, to shape, to where protection and padding are distributed.
Speed is another factor that can change our gait. From the gentle stroll at an art gallery to professional sprinters, speed changes the way we move. In the next and probably final chapter of this series on gait, we will take a last loop on the walking cycle to see the subtle variations we go through as we speed up our steps, and we'll finally tackle something that has been silently missing from these articles: running.
YOU MAY ALSO ENJOY:
With the knowledge of the previous posts put together, I would like to cover why we tend to anticipate actions. Why does going backward help us move forward, why does going down help us go up, and how does this counterintuitive idea of going in the opposite direction make us move more efficiently?


Bibliography and references
Perry, Jaquelin. Gait Analysis - Normal and Pathological Function.
Rose, Jessica. Gamble, James G. Human Walking.
Palastanga, Nigel. Field, Derek. Soames, Roger. Anatomy and Human Movement.
Vaughan, Christopher L. Davis, Brian L. O’connor, Jeremy C. Dynamics of Human Gait.
Ferber, Reed. Macdonald, Shari. Running Mechanics and Gait Analysis.
Yegian, Andrew K. The Role of Muscles in Arm Swing and Thoracic Rotation During Walking
Desilva, Jeremy. First Steps: How Upright Walking Made Us Human.
Thomas K. Uchida, Scott L. Delp: Biomechanics of movement.
Andreas Mayer: The Science of Walking.
Earls, James. Born to Walk.
Arm swing in human locomotion
https://en.wikipedia.org/wiki/Arm_swing_in_human_locomotion
Biomechanics Lecture 11: Gait
https://www.youtube.com/watch?v=QB0tJajDvMw&list=PLS-ocxImwSG_VODKg-Ow12FsyGfDC9cnz&index=11
Observational Gait Analysis - Lecture 1
https://www.youtube.com/watch?v=WsnWnvH3PrM&list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Observational Gait Analysis - Case Study Review
https://youtu.be/USEtXSRkfAU?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
THE PHASES OF WALKING (GAIT CYCLE BREAKDOWN)
https://youtu.be/QAnEhz6Eqn4?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Phases of the Gait Cycle 1
https://youtu.be/JM0EwSlvR1c?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Explaining the Gait Cycle for the NPTE
https://youtu.be/dvpi1WHCDwM?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Ground Reaction Force During the Gait Cycle
https://youtu.be/Y2RHvicAM2o?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Analysis of Gait Motion Frontal Plane
https://youtu.be/SV0dQnimzrg?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Analysis of Gait Motion: Transverse Plane
https://youtu.be/H4wXKqmJac4?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Analysis of Gait Motion: Sagittal Plane
https://youtu.be/uh7riepyJl4?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Athletic Male Standard Walk - Realtime. Animation Reference Body Mechanics
https://youtu.be/GBkJY86tZRE?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
The Gait Cycle
https://youtu.be/-G3EFtkq3qI?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Walking Gait Analysis, In Sagital, Frontal and Transverse plane ||Gait Biomechanics
https://youtu.be/OcLFMHTyrnw?list=PLwSMRX38xS9AVhulUENkZLCraUn3GM6x3
Athletic Male Standard Walk. Animation Reference Body Mechanics
https://youtu.be/vq9A5FD8G5w
The Catapult Mechanism: Elastic Recoil of Fascial Tissues
https://fasciatrainingacademy.com/the-catapult-mechanism-elastic-recoil-of-fascial-tissues/
Foot and Ankle Structure and Function
https://www.physio-pedia.com/Foot_and_Ankle_Structure_and_Function
The Gait Cycle
https://www.physio-pedia.com/The_Gait_Cycle
Muscle Activity During Gait
https://www.physio-pedia.com/Muscle_Activity_During_Gait
See how the muscles work to create ambulation
https://canada.humankinetics.com/blogs/excerpt/see-how-the-muscles-work-to-create-ambulation?utm_
TRENDELENBURG GAIT material:
Trendelenburg Gait: Causes, Symptoms, and Role of the Gluteus Medius :
https://youtu.be/-Xh0B2XhK3s
Trendelenburg Sign - Everything You Need To Know - Dr. Nabil Ebraheim
https://youtu.be/Jn4mpfatnjY
Trendelenburg Gait: Explained
https://youtu.be/6VdnNm4nNHg
Online articles:
https://www.physio-pedia.com/Trendelenburg_Gait
https://www.ncbi.nlm.nih.gov/books/NBK541094/
https://en.wikipedia.org/wiki/Trendelenburg_gait
https://crouchphysio.com/understanding-trendelenburg-gait-a-physiotherapists-perspective/
https://en.wikipedia.org/wiki/Trendelenburg%27s_sign
https://my.clevelandclinic.org/health/diseases/21092-gait-disorders
ATAXIC GAIT:
https://www.mayoclinic.org/diseases-conditions/ataxia/symptoms-causes/syc-20355652
https://www.physio-pedia.com/Ataxia
https://protokinetics.com/common-gait-deviations-ataxic-gait/
https://my.clevelandclinic.org/health/symptoms/17748-ataxia
https://en.wikipedia.org/wiki/Ataxia
ANTALGIC GAIT:
https://www.webmd.com/pain-management/what-is-antalgic-gait
https://www.healthline.com/health/antalgic-gait#takeaway
https://www.physio-pedia.com/Gait:_Antalgic
https://www.physio-pedia.com/Gait_Deviations?utm_source=physiopedia&utm_medium=related_articles&utm_campaign=ongoing_internal
https://www.physio-pedia.com/Paediatric_Limping_Gait?utm_source=physiopedia&utm_medium=related_articles&utm_campaign=ongoing_internal
https://en.wikipedia.org/wiki/Antalgic_gait
STEPPAGE GAIT:
https://mdsearchlight.com/joint-muscle-and-bone/steppage-gait/
https://www.ncbi.nlm.nih.gov/books/NBK547672/
https://www.sciencedirect.com/topics/veterinary-science-and-veterinary-medicine/steppage-gait
https://en.wikipedia.org/wiki/Foot_drop
https://en.wikipedia.org/wiki/Steppage_gait
In this piece, we will cover some of the most common deviations from the "standard" walk, see both what happens when parts of the system fail, and how the body tries to adapt around it.